
It’s 10:34 PM on a Friday. A hobby powerlifter, 94 kilograms, finishes his second heavy session of the week. Bench press 105 kg for 5×3, followed by paused squats at 100 kg. Classic block periodization push.
He goes home. Showers. Reads briefly on the couch. Goes to bed. Subjectively, a normal evening.
What he doesn’t know: his blood sugar at this moment is 78 mg/dL — and falling. An hour later it will be at 68 mg/dL. Three hours later, 60 mg/dL. He’ll spend the next four hours stuck in a mild, persistent hypoglycemia.
His Whoop will record a Sleep Performance of 72% that night — the lowest reading of the entire week. REM sleep just 26 minutes, sleep efficiency reduced.
But subjectively? An “okay” night.
This phenomenon — the gap between subjective experience and actual physiological state — is exactly why Continuous Glucose Monitoring (CGM) is becoming an increasingly relevant tool for athletes. Even athletes without any metabolic disease.
In this article we walk through two real, recorded training sessions of an anonymized hobby athlete to show how dramatically the glucose response can differ at comparable training volumes — and what role pre-workout meal, training demand, and intra-workout carbs play.
Methodological note: The data presented here comes from one individual, two sessions, March 2026, recorded with a FreeStyle Libre 3. This is a case description, not a study. The mechanisms are physiologically established; whether the specific patterns generalize to other athletes cannot be inferred from this.
The Athlete and the Setup
- Sex / age: male, mid-30s
- Bodyweight: 94 kg, lean bulk
- Training level: ambitious hobby powerlifter, multiple years of experience
- Programming: block periodization, in tapering block (5×5 → 4×2 → 3×2 depending on lift)
- Training splits: squat / bench / deadlift focus days with multiple accessories — effectively full-body due to volume
- Training-day nutrition: structured meals throughout the day, no fasted lifting
- Intra-workout (identical both sessions): 60 g maltodextrin + 25 g clear whey in water
- No pre-workout booster, no caffeine stack during the test window
- CGM: FreeStyle Libre 3, exported via LibreView, 1-minute resolution
Session 1: Wednesday, March 3rd, 2026 — the spike to 225 mg/dL
The day’s timeline
| Time | Meal / Event |
|---|---|
| 08:00 | Breakfast 1: 500 g Skyr |
| 10:00 | Breakfast 2: 2 whole eggs + 2 egg whites |
| ~13:00 | Lunch: chicken + rice + vegetables |
| 15:30 | Pre-workout snack: oatmeal with milk + chia |
| 16:24 | Training start (squat-focused lower-heavy + push) |
The session
- Backsquat 140 kg, 3×4 (main lift)
- Romanian Deadlifts 110 kg, 3×8
- Paused Bench Press 90 kg, 4×5
- Seated Leg Extensions 70 kg, 3×12
- Incline Biceps Curls 2×20 kg, 3×10
- Hanging Leg Raises 3×20
Whoop training strain: 12.9 | Duration: 112 min | Max-HR: 138
Backsquat plus Romanian Deadlifts in the same session means maximum muscle mass recruitment — these are the two lifts with the highest glycogen demand per rep. The athlete entered with well-stocked stores (Skyr + eggs + lunch + oat snack). Pre-workout glucose: 98 mg/dL.
What the CGM showed
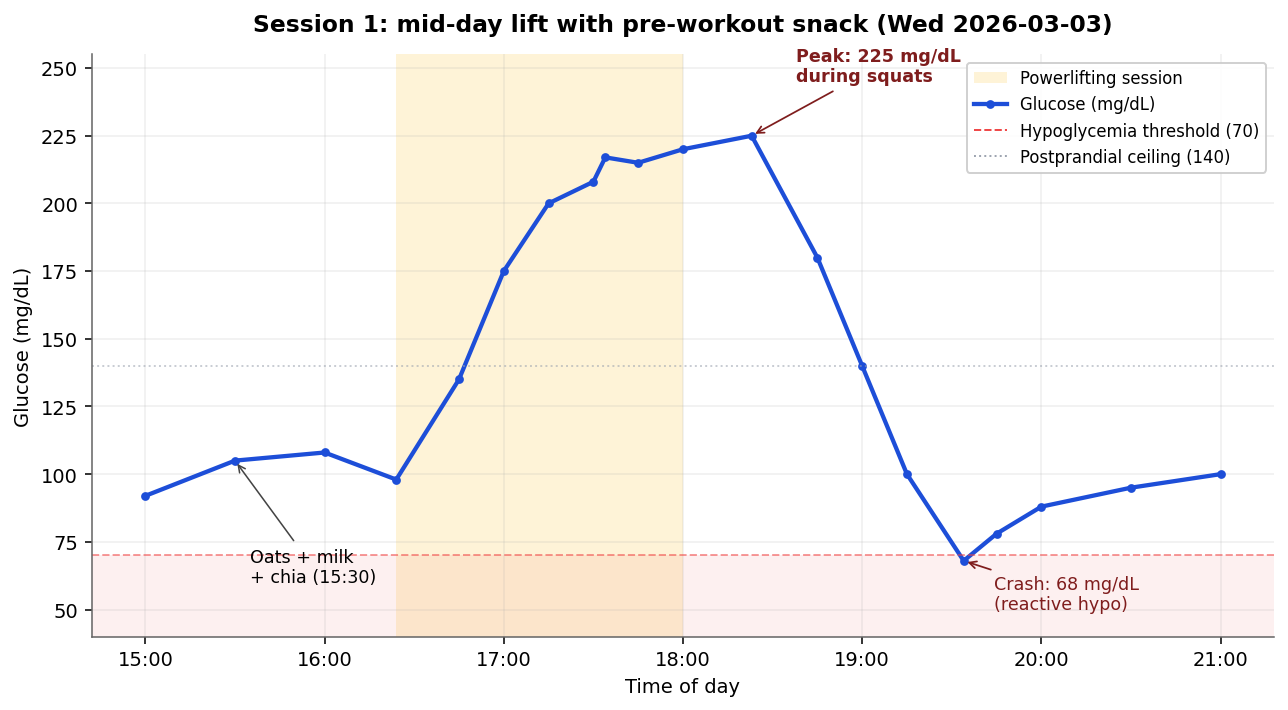
From the first sip of intra-workout solution, blood sugar rises sharply:
- 16:24 Workout start, 98 mg/dL
- 17:30 during backsquats: 208 mg/dL
- 17:34 Peak: 217 mg/dL
- 18:23 during RDLs: 225 mg/dL — daily high
- 18:00 Workout end, sharp decline begins
- 19:34 Crash to 68 mg/dL
That’s a swing of 157 mg/dL in under two hours, with a reactive hypoglycemia ~30 minutes post-workout.
Why so high?
Three factors compound:
- 60 g of fast carbs (maltodextrin) hitting an already filled metabolism.
- Adrenaline and cortisol during heavy squat sets temporarily blunt insulin action — the body throttles glucose uptake into muscle to keep blood glucose available for fight-or-flight. This is exercise-induced insulin resistance (Sigal et al., 1994).
- The oat snack 50 minutes prior was a light carb hit with little protein/fat — minimal brake, fast availability.
After the last set, sympathetic tone drops, insulin acts at full capacity again — and aggressively clears the elevated glucose. Result: reactive hypoglycemia.
Session 2: Friday, March 5th, 2026 — the invisible crash
The day’s timeline
| Time | Meal / Event |
|---|---|
| 19:00 | Pre-workout meal: 50 g rice + 150 g chicken + vegetables |
| 20:45 | Training start (bench-focused upper + light squat) |
| 22:11 | Training end |
| After | No further food, straight to bed |
The session
- Bench 105 kg, 5×3 (main lift)
- Paused Back Squat 100 kg, 4×4 (volume, not max)
- Seated DB Shoulder Press 2×28 kg, 3×10
- Lateral Raise 2×12.5 kg, 3×15
- Triceps Pushdown 80 kg, 3×12
- Facepulls 105 kg, 3×10
Whoop training strain: 12.9 | Duration: 86 min | Max-HR: 136
Same Whoop strain as Session 1 — but substantially lower glycogen demand: no RDL, the squat was a paused variant at submaximal load, the rest was upper body with more isolation work.
What the CGM showed
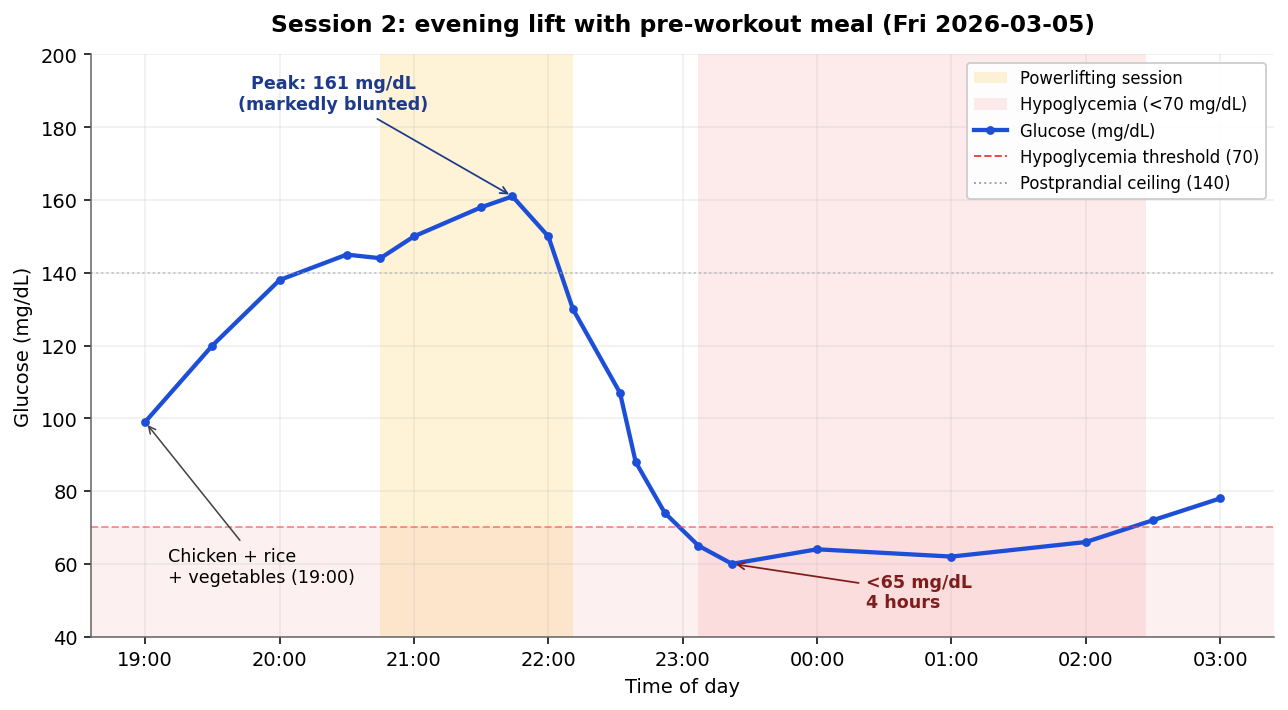
- 19:00 Pre-workout meal, glucose ~99 mg/dL
- 19:00–20:45 gentle rise to 145 mg/dL via rice digestion
- 20:45 Workout start
- 21:44 Peak: 161 mg/dL — markedly damped vs. Session 1
- 22:11 Workout end
- 22:32 Glucose at 107 mg/dL
- 22:39 below 90 mg/dL
- 22:52 below 75 mg/dL
- 23:07 65 mg/dL, beginning of the four-hour hypoglycemia
- 23:22 60 mg/dL — lowest point
- 00:00 still 64 mg/dL
Glucose remained below 70 mg/dL from 23:07 until 02:30 — over four hours in the hypoglycemic range.
Why so flat in the lift, so deep at night?
During the lift:
- Rice + chicken + vegetables is a matrix of resistant starch, protein, and fiber. It slows glucose absorption.
- Lower training demand = smaller cortisol/adrenaline surge.
- The maltodextrin was therefore taken up primarily by working muscle, not “parked” in the bloodstream.
After the lift:
- Insulin is mobilized (from meal + malto).
- Glycogen reload continues to pull glucose out of the blood.
- No new carbs come in (no post-workout snack, straight to bed).
Result: a continuous glucose drift into hypo territory that persists for hours.
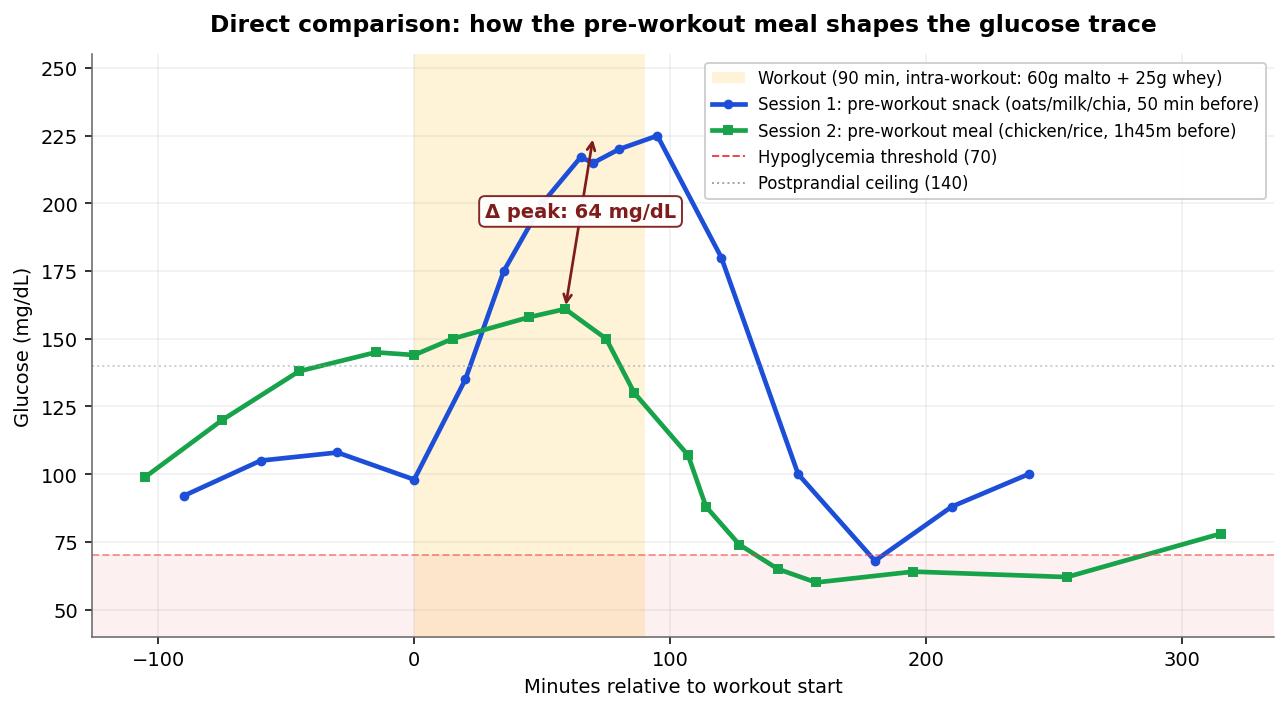
Direct comparison
| Parameter | Session 1 | Session 2 |
|---|---|---|
| Pre-workout meal | Oat snack (50 min before) | Rice + chicken (1:45 h before) |
| Pre-workout glucose | 98 mg/dL | 99 mg/dL |
| Intra-workout | 60 g malto + 25 g whey | 60 g malto + 25 g whey |
| Peak in lift | 225 mg/dL | 161 mg/dL |
| Training focus | Squat + RDL (high demand) | Bench + light squat |
| Whoop strain | 12.9 | 12.9 |
| Post-workout meal | Late dinner | None |
| Crash to | 68 mg/dL | 60 mg/dL |
| Hypo duration | ~10 min | ~4 hours |
Δ Peak: 64 mg/dL — at identical intra-workout strategy. Pre-workout setup and training demand made the difference.
The Whoop signal: what the sleep tells us
The night after Session 2, the athlete spent ~4 hours in mild hypoglycemia. What does Whoop show?
| Night | Sleep Performance | REM | In bed | Disturbances |
|---|---|---|---|---|
| Wed → Thu (after Session 1) | 79% | 42 min | 6:48 h | 11 |
| Thu → Fri | 84% | 99 min | 8:12 h | 18 |
| Fri → Sat (after Session 2) | 72% | 26 min | 5:48 h | 5 |
| Sat → Sun | 84% | 100 min | 7:36 h | 8 |
The night after Session 2 is clearly the outlier — particularly in REM sleep (26 vs. 42–100 minutes in other nights). This fits the physiology: hypoglycemia activates the sympathetic nervous system, REM sleep requires parasympathetic dominance. The two states are incompatible.
Subjectively? An okay night.
That’s the punchline: CGM and wearable, taken together, surfaced a physiological event that would have remained invisible without these tools — and that likely degraded recovery scores, HRV, and the next day’s training over weeks.
What can we take from this?
If you use intra-workout carbs in strength training, three takeaways matter:
1. The pre-workout meal is not a detail
Same carbs, same whey, same strain — but the spike differed by 64 mg/dL. A complex, fiber-rich meal 60–120 minutes before the lift markedly damps peak glucose. A fast snack right before pushes you higher.
2. If you carb during the lift, eat after it
Session 2 demonstrates: without a post-workout meal, you drive yourself into a multi-hour hypoglycemia. Not acutely dangerous (for metabolically healthy individuals), but it costs sleep quality. A small meal (20–40 g carbs + protein) within 30 minutes of finishing the lift catches the crash.
3. Late-evening lifting + intra-workout carbs is a poor combination
If the athlete sleeps right after the lift, the hypo phase becomes the sleep phase. Sympathetic activation from low blood glucose disrupts REM sleep — visible in the Whoop trace. Late-evening lifters should either reduce intra-workout carbs or schedule a post-workout snack, hungry or not.
Methodological limits
- N=2 sessions in a single sensor window. This is a case description, not a study.
- CGM measures interstitial fluid, not direct blood — meaning a 5–15 minute lag vs. actual blood glucose.
- Confounders: sleep quality is influenced by many variables (room temperature, stress, meal timing). The correlation to hypo duration is plausible, not causally proven.
- Individual variation: insulin sensitivity, glycogen storage, and cortisol response vary substantially between people. Other athletes might experience these sessions very differently.
FAQ
Does blood sugar rise during strength training?
Yes, through two mechanisms: (1) adrenaline and cortisol during intense sets release glucose from glycogen stores; (2) if intra-workout carbs are consumed, they add on top. How high the spike goes depends heavily on the pre-workout meal and training intensity.
What is reactive hypoglycemia?
A glucose crash below ~70 mg/dL following a prior spike. Caused by an insulin response that continued to act after the spike, even though the original glucose source (meal, malto) has been cleared. In metabolically healthy individuals it’s rarely dangerous, but can cause fatigue, focus issues, and disrupted sleep.
Do I need a CGM as a hobby athlete?
No — but it’s a precise diagnostic tool. A CGM costs ~€65–95 for 14 days. If you want to know how your own metabolism responds to specific meal/training combinations, you get data you can’t otherwise obtain. For 2–4 weeks per quarter it’s a sensible investment for ambitious athletes — see also our FreeStyle Libre 3 review.
What’s a “normal” glucose level after exercise?
In metabolically healthy people the value should return below 140 mg/dL within 1–2 hours of exercise. Acute spikes above 180 mg/dL during intense sets aren’t pathological — they reflect the stress response, not insulin resistance. Sustained elevation over 2+ hours warrants a conversation with a physician.
Are intra-workout carbs (maltodextrin) worth it?
For sessions over 60–90 minutes and/or with high glycogen demand: yes, they can improve performance and recovery (Burke et al., 2011). But this article shows: if you use them, don’t skip the post-workout meal — otherwise the reactive hypo phase costs more than the carbs deliver.
What’s next
The data shown here is a pilot. A follow-up phase is planned with 4–6 weeks of continuous CGM recording, in which different pre- and post-workout strategies will be tested against the same training templates. If you’re interested in the topic: the next update will cover HRV correlations, recovery scores, and whether a post-workout carb snack actually catches the hypo phase.
Sources & further reading
- Sigal RJ, Purdon C, Fisher SJ, et al. Hyperinsulinemia prevents prolonged hyperglycemia after intense exercise in insulin-dependent diabetic subjects. J Clin Endocrinol Metab. 1994.
- Burke LM, Hawley JA, Wong SH, Jeukendrup AE. Carbohydrates for training and competition. J Sports Sci. 2011.
- Marliss EB, Vranic M. Intense exercise has unique effects on both insulin release and its roles in glucoregulation. Diabetes. 2002.
- Borer KT. Advanced Exercise Endocrinology. Human Kinetics. 2014.
Keep reading
Related articles on this topic: